
Isolated and Combined Effect of Age and Gender on Neutrophil–Lymphocyte Ratio in the Hyperglycemic Saudi Population

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
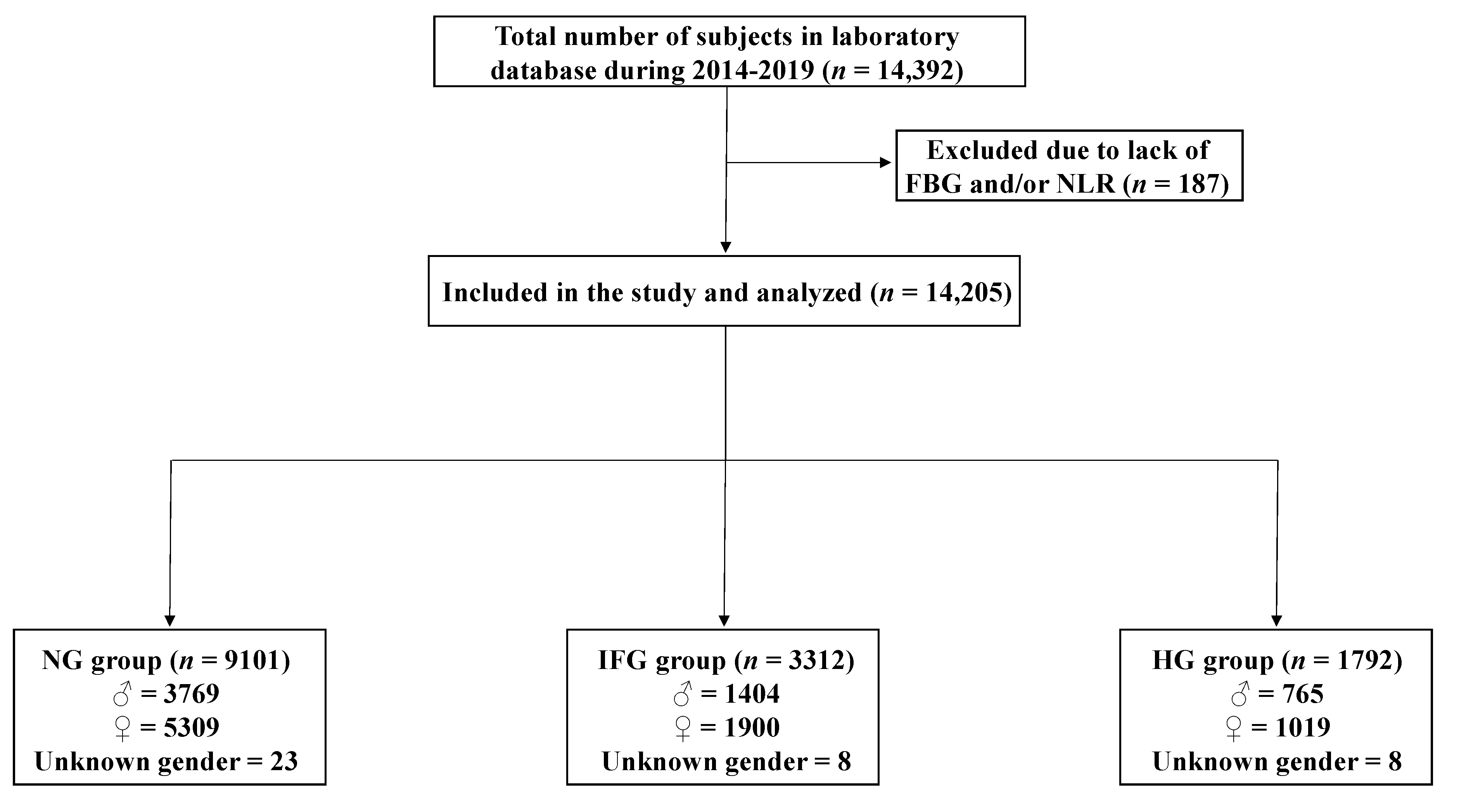
2.1. Study Design, Population, and Data Collection
2.2. Statistical Analysis
3. Results
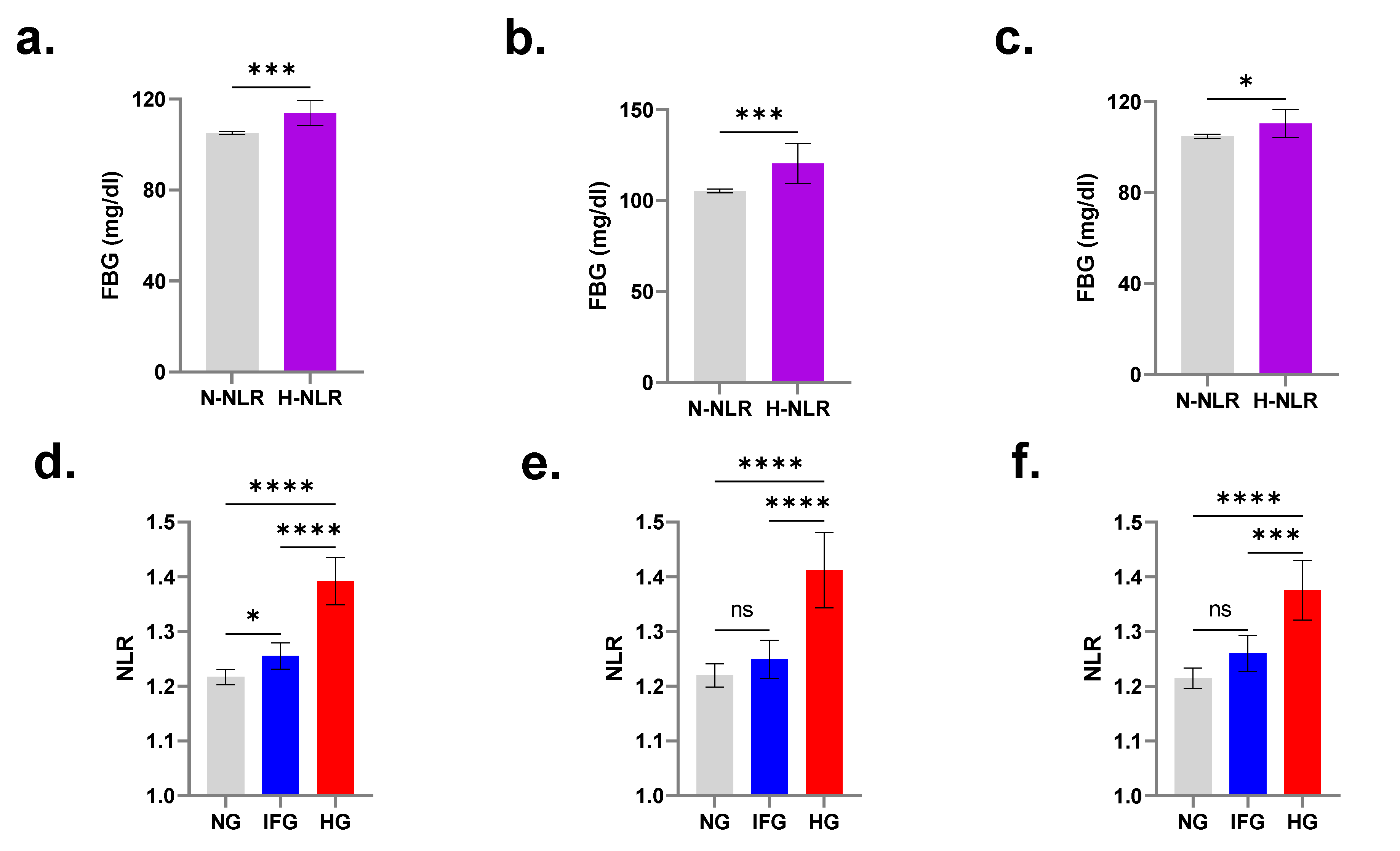
3.1. FBG Is Significantly Increased in Individuals with Elevated NLR
3.2. Subjects with IFG and HG Have Significantly Elevated NLR
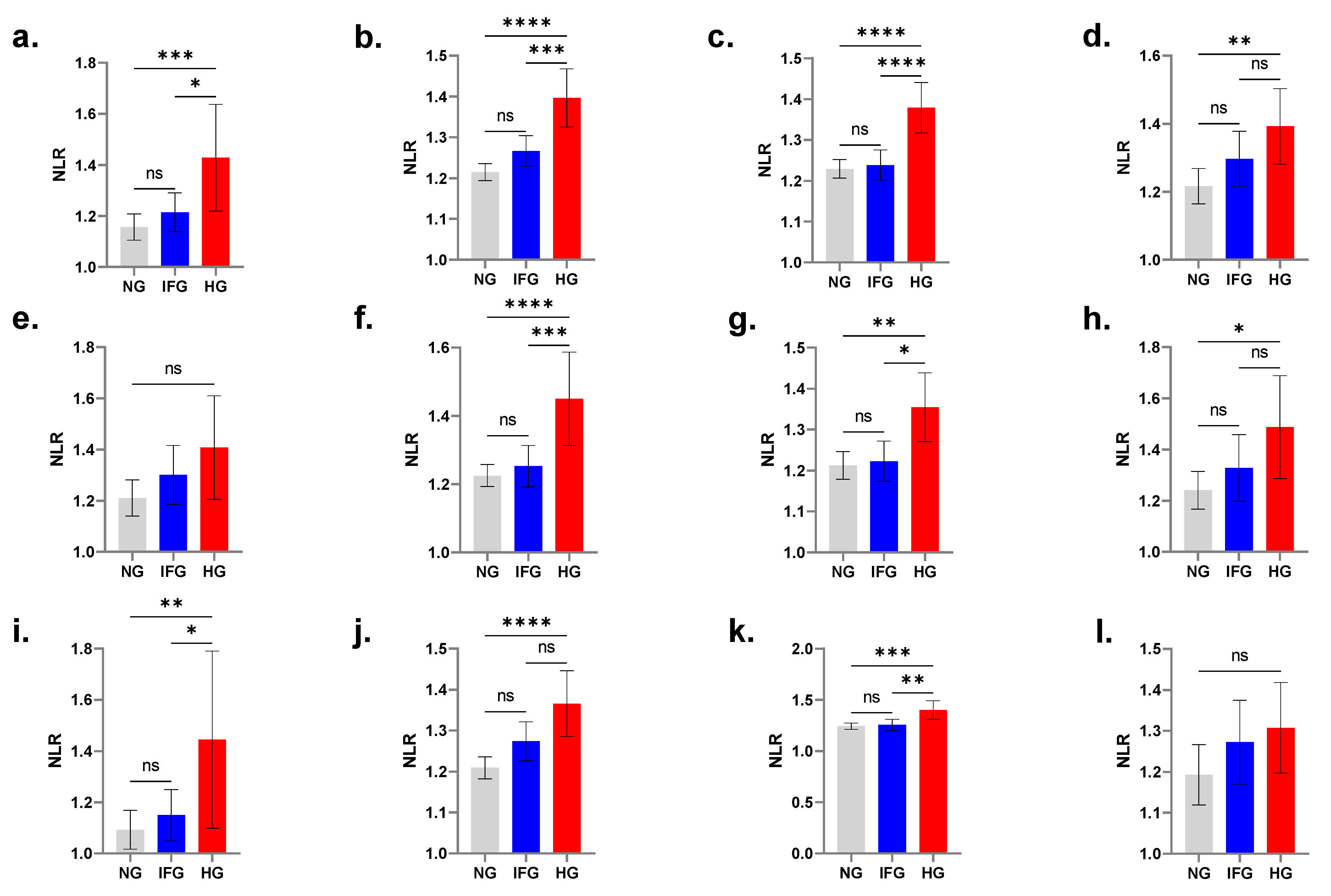
3.3. Age-Controlled Comparisons Displace NLR Significance in IFG
3.4. NLR Is Not Elevated in Hyperglycemic Young Males
3.5. NLR Is Not Elevated in Hyperglycemic Elderly Females
3.6. Elevated NLR Is More Prevalent in HG Subjects
3.7. Elevated NLR Carries a Greater Risk for HG
3.8. Correlation between NLR and FBG
3.9. NLR Displays Poor Diagnostic Accuracy for HG
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care 2014, 37 (Suppl. S1), S14–S80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inzucchi, S.E. Diagnosis of diabetes. N. Engl. J. Med. 2013, 368, 193. [Google Scholar] [CrossRef] [PubMed]
- Al-Rubeaan, K.; Siddiqui, K.; Saeb, A.T.; Nazir, N.; Al-Naqeb, D.; Al-Qasim, S. ACE I/D and MTHFR C677T polymorphisms are significantly associated with type 2 diabetes in Arab ethnicity: A meta-analysis. Gene 2013, 520, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Al-Nozha, M.M.; Al-Hazzaa, H.M.; Arafah, M.R.; Al-Khadra, A.; Al-Mazrou, Y.Y.; Al-Maatouq, M.A.; Khan, N.B.; Al-Marzouki, K.; Al-Harthi, S.S.; Abdullah, M.; et al. Prevalence of physical activity and inactivity among Saudis aged 30–70 years. A population-based cross-sectional study. Saudi Med. J. 2007, 28, 559–568. [Google Scholar] [PubMed]
- Mahfouz, A.A.; Abdelmoneim, I.; Khan, M.Y.; Daffalla, A.A.; Diab, M.M.; Al-Gelban, K.S.; Moussa, H. Obesity and Related Behaviors among Adolescent School Boys in Abha City, Southwestern Saudi Arabia. J. Trop. Pediatr. 2007, 54, 120–124. [Google Scholar] [CrossRef] [Green Version]
- Bassiony, M.M. Smoking in Saudi Arabia. Saudi Med. J. 2009, 30, 876–881. [Google Scholar]
- Goldberg, R.B. Cytokine and Cytokine-Like Inflammation Markers, Endothelial Dysfunction, and Imbalanced Coagulation in Development of Diabetes and Its Complications. J. Clin. Endocrinol. Metab. 2009, 94, 3171–3182. [Google Scholar] [CrossRef] [Green Version]
- Bailes, B.K. Diabetes mellitus and its chronic complications. AORN J. 2002, 76, 265–282. [Google Scholar] [CrossRef] [Green Version]
- Feuerer, M.; Shen, Y.; Littman, D.R.; Benoist, C.; Mathis, D. How Punctual Ablation of Regulatory T Cells Unleashes an Autoimmune Lesion within the Pancreatic Islets. Immunity 2009, 31, 654–664. [Google Scholar] [CrossRef] [Green Version]
- Rendra, E.; Riabov, V.; Mossel, D.M.; Sevastyanova, T.; Harmsen, M.C.; Kzhyshkowska, J. Reactive oxygen species (ROS) in macrophage activation and function in diabetes. Immunobiology 2018, 224, 242–253. [Google Scholar] [CrossRef]
- Tsalamandris, S.; Antonopoulos, A.S.; Oikonomou, E.; Papamikroulis, G.-A.; Vogiatzi, G.; Papaioannou, S.; Deftereos, S.; Tousoulis, D. The Role of Inflammation in Diabetes: Current Concepts and Future Perspectives. Eur. Cardiol. Rev. 2019, 14, 50–59. [Google Scholar] [CrossRef] [Green Version]
- Schuster, D. Obesity and the development of type 2 diabetes: The effects of fatty tissue inflammation. Diabetes, Metab. Syndr. Obesity: Targets Ther. 2010, 3, 253–262. [Google Scholar] [CrossRef] [Green Version]
- Vozarova, B.; Weyer, C.; Lindsay, R.S.; Pratley, R.E.; Bogardus, C.; Tataranni, P.A. High White Blood Cell Count Is Associated With a Worsening of Insulin Sensitivity and Predicts the Development of Type 2 Diabetes. Diabetes 2002, 51, 455–461. [Google Scholar] [CrossRef] [Green Version]
- Azab, B.; Jaglall, N.; Atallah, J.P.; Lamet, A.; Raja-Surya, V.; Farah, B.; Lesser, M.; Widmann, W.D. Neutrophil-Lymphocyte Ratio as a Predictor of Adverse outcomes of Acute Pancreatitis. Pancreatology 2011, 11, 445–452. [Google Scholar] [CrossRef]
- Hajibandeh, S.; Hajibandeh, S.; Hobbs, N.; Mansour, M. Neutrophil-to-lymphocyte ratio predicts acute appendicitis and distinguishes between complicated and uncomplicated appendicitis: A systematic review and meta-analysis. Am. J. Surg. 2020, 219, 154–163. [Google Scholar] [CrossRef] [Green Version]
- Lowsby, R.; Gomes, C.; Jarman, I.; Lisboa, P.; Nee, P.A.; Vardhan, M.; Eckersley, T.; Saleh, R.; Mills, H. Neutrophil to lymphocyte count ratio as an early indicator of blood stream infection in the emergency department. Emerg. Med. J. 2014, 32, 531–534. [Google Scholar] [CrossRef] [Green Version]
- Lo, Y.T.; Lim, V.Y.; Ng, M.; Tan, Y.H.; Chiang, J.; Chang, E.W.Y.; Chan, J.Y.; Poon, E.Y.L.; Somasundaram, N.; Rashid, M.F.B.H.; et al. A Prognostic Model Using Post-Steroid Neutrophil-Lymphocyte Ratio Predicts Overall Survival in Primary Central Nervous System Lymphoma. Cancers 2022, 14, 1818. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Ma, J.; Jiang, Z.; Ming, L. Prognostic value of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in acute pulmonary embolism: A systematic review and meta-analysis. Int. Angiol. 2018, 37, 4–11. [Google Scholar] [CrossRef]
- Chua, W.; Charles, K.A.; Baracos, V.E.; Clarke, S.J. Neutrophil/lymphocyte ratio predicts chemotherapy outcomes in patients with advanced colorectal cancer. Br. J. Cancer 2011, 104, 1288–1295. [Google Scholar] [CrossRef] [Green Version]
- Forget, P.; Khalifa, C.; Defour, J.P.; Latinne, D.; Van Pel, M.C.; De Kock, M. What is the normal value of the neutrophil-to-lymphocyte ratio? BMC Res. Notes 2017, 10, 12. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Liu, Y.; Xiang, P.; Pu, L.; Xiong, H.; Li, C.; Zhang, M.; Tan, J.; Xu, Y.; Song, R.; et al. Neutrophil-to-lymphocyte ratio predicts critical illness patients with 2019 coronavirus disease in the early stage. J. Transl. Med. 2020, 18, 206. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.-Y.; Kim, H.-N.; Lee, S.H.; Kim, S.J.; Chang, Y.; Ryu, S.; Shin, H.; Kim, H.-L.; Lee, J.H. Association between Neutrophil-to-Lymphocyte Ratio and Gut Microbiota in a Large Population: A Retrospective Cross-Sectional Study. Sci. Rep. 2018, 8, 16031. [Google Scholar] [CrossRef]
- Huang, J.; Xiao, Y.; Xu, A.; Zhou, Z. Neutrophils in type 1 diabetes. J. Diabetes Investig. 2015, 7, 652–663. [Google Scholar] [CrossRef]
- Duman, T.T.; Aktas, G.; Atak, B.M.; Kocak, M.Z.; Erkus, E.; Savli, H. Neutrophil to lymphocyte ratio as an indicative of diabetic control level in type 2 diabetes mellitus. Afr. Health Sci. 2019, 19, 1602–1606. [Google Scholar] [CrossRef]
- Dowey, R.; Iqbal, A.; Heller, S.R.; Sabroe, I.; Prince, L.R. A Bittersweet Response to Infection in Diabetes; Targeting Neutrophils to Modify Inflammation and Improve Host Immunity. Front Immunol. 2021, 12, 678771. [Google Scholar] [CrossRef]
- Guerrero-Hernandez, A.; Verkhratsky, A. Calcium signalling in diabetes. Cell Calcium 2014, 56, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Gorroño, L.E.; López-Díez, R.; Yepuri, G.; Ramirez, L.S.; Reverdatto, S.; Gugger, P.; Shekhtman, A.; Ramasamy, R.; Schmidt, A.M. Receptor for Advanced Glycation End Products (RAGE) and Mechanisms and Therapeutic Opportunities in Diabetes and Cardiovascular Disease: Insights From Human Subjects and Animal Models. Front. Cardiovasc. Med. 2020, 7, 37. [Google Scholar] [CrossRef]
- Al Mamun, A.; Wu, Y.; Nasrin, F.; Akter, A.; Taniya, M.A.; Munir, F.; Jia, C.; Xiao, J. Role of Pyroptosis in Diabetes and Its Therapeutic Implications. J. Inflamm. Res. 2021, 14, 2187–2206. [Google Scholar] [CrossRef] [PubMed]
- Sefil, F.; Ulutaş, K.T.; Dokuyucu, R.; Sumbul, A.T.; Yengil, E.; Yagiz, A.E.; Yula, E.; Ustun, I.; Gokce, C. Investigation of neutrophil lymphocyte ratio and blood glucose regulation in patients with type 2 diabetes mellitus. J. Int. Med Res. 2014, 42, 581–588. [Google Scholar] [CrossRef]
- Akbas, E.M.; Demirtas, L.; Ozcicek, A.; Timuroglu, A.; Bakirci, E.M.; Hamur, H.; Ozcicek, F.; Turkmen, K. Association of epicardial adipose tissue, neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio with diabetic nephropathy. Int. J. Clin. Exp. Med. 2014, 7, 1794–1801. [Google Scholar]
- Wang, R.T.; Zhang, J.R.; Li, Y.; Liu, T.; Yu, K.J. Neutrophil-Lymphocyte ratio is associated with arterial stiffness in diabetic retinopathy in type 2 diabetes. J. Diabetes Complicat. 2015, 29, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Zou, S.; Wang, C.; Tan, X.; Yu, M. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio in Chinese Han population from Chaoshan region in South China. BMC Cardiovasc. Disord. 2019, 19, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simental-Mendía, L.E.; Lazalde, B.; Zambrano-Galván, G.; Simental-Saucedo, L.; Rábago-Sánchez, E.; Rodríguez-Morán, M.; Guerrero-Romero, F. Relation Between C-Reactive Protein and Impaired Fasting Glucose in Obese Subjects. Inflammation 2012, 35, 1742–1746. [Google Scholar] [CrossRef] [PubMed]
- Chakarova, N.; Tankova, T.; Atanassova, I.; Dakovska, L. Serum lipid and hsCRP levels in prediabetes—impaired fasting glucose (IFG) and impaired glucose tolerance (IGT). Diabetes Res. Clin. Pract. 2009, 86, 56–60. [Google Scholar] [CrossRef]
- Tramunt, B.; Smati, S.; Grandgeorge, N.; Lenfant, F.; Arnal, J.-F.; Montagner, A.; Gourdy, P. Sex differences in metabolic regulation and diabetes susceptibility. Diabetologia 2019, 63, 453–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erbaş, I.M.; Hajikhanova, A.; Besci, O.; Acinikli, K.Y.; Demir, K.; Böber, E.; Abacı, A. Initial neutrophil/lymphocyte and lymphocyte/monocyte ratios can predict future insulin need in newly diagnosed type 1 diabetes mellitus. J. Pediatr. Endocrinol. Metab. 2022, 35, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Grumbach, M.M.; Auchus, R.J. Estrogen: Consequences and Implications of Human Mutations in Synthesis and Action1. J. Clin. Endocrinol. Metab. 1999, 84, 4677–4694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anagnostis, P.; Christou, K.; Artzouchaltzi, A.-M.; Gkekas, N.; Kosmidou, N.; Siolos, P.; Paschou, S.A.; Potoupnis, M.; Kenanidis, E.; Tsiridis, E.; et al. Early menopause and premature ovarian insufficiency are associated with increased risk of type 2 diabetes: A systematic review and meta-analysis. Eur. J. Endocrinol. 2019, 180, 41–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanaya, A.M.; Herrington, D.; Vittinghoff, E.; Lin, F.; Grady, D.; Bittner, V.; Cauley, J.A.; Barrett-Connor, E. Glycemic Effects of Postmenopausal Hormone Therapy: The Heart and Estrogen/progestin Replacement Study: A Randomized, Double-Blind, Placebo-Controlled Trial. Ann. Intern. Med. 2003, 138, 1–9. [Google Scholar] [CrossRef]
- Margolis, K.L.; Bonds, D.E.; Rodabough, R.J.; Tinker, L.; Phillips, L.S.; Allen, C.; Bassford, T.; Burke, G.; Torrens, J.; Howard, B.V. Effect of oestrogen plus progestin on the incidence of diabetes in postmenopausal women: Results from the Women’s Health Initiative Hormone Trial. Diabetologia 2004, 47, 1175–1187. [Google Scholar] [CrossRef]
- Al-Rubeaan, K.; Al-Manaa, H.; Khoja, T.; Ahmad, N.; Al-Sharqawi, A.; Siddiqui, K.; AlNaqeb, D.; Aburisheh, K.; Youssef, A.; Al-Batil, A.; et al. The Saudi Abnormal Glucose Metabolism and Diabetes Impact Study (SAUDI-DM). Ann. Saudi Med. 2014, 34, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Demirtas, L.; Degirmenci, H.; Akbas, E.M.; Ozcicek, A.; Timuroglu, A.; Gurel, A.; Ozcicek, F. Association of hematological indicies with diabetes, impaired glucose regulation and microvascular complications of diabetes. Int. J. Clin. Exp. Med. 2015, 8, 11420–11427. [Google Scholar] [PubMed]
- Pollack, R.M.; Donath, M.Y.; Leroith, D.; Leibowitz, G. Anti-inflammatory Agents in the Treatment of Diabetes and Its Vascular Complications. Diabetes Care 2016, 39 (Suppl. 2), S244–S252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, P.; Li, R.; Yu, S.; Xu, T.; Yue, S.; Ji, Y.; Chen, X.; Xie, H. The Relationship between Neutrophil-to-Lymphocyte Ratio and Intracerebral Hemorrhage in Type 2 Diabetes Mellitus. J. Stroke Cerebrovasc. Dis. 2016, 26, 930–937. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zheng, H.; Zhu, X.; Mao, F.; Zhang, S.; Shi, H.; Li, Y.; Lu, B. Neutrophil-to-lymphocyte ratio is associated with diabetic peripheral neuropathy in type 2 diabetes patients. Diabetes Res. Clin. Pract 2017, 130, 90–97. [Google Scholar] [CrossRef]
- Atli, H.; Onalan, E.; Yakar, B.; Duzenci, D.; Donder, E. Predictive value of inflammatory and hematological data in diabetic and non-diabetic retinopathy. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 76–83. [Google Scholar] [PubMed]
- Cheng, Y.; Yu, W.; Zhou, Y.; Zhang, T.; Chi, H.; Xu, C. Novel predictor of the occurrence of DKA in T1DM patients without infection: A combination of neutrophil/lymphocyte ratio and white blood cells. Open Life Sci. 2021, 16, 1365–1376. [Google Scholar] [CrossRef]
- Wen, H.; Yu, H. Correlation analysis of carotid plaque in young patients with newly diagnosed type 2 diabetes and platelet-to-lymphocyte ratio and neutrophil–lymphocyte ratio. Vascular 2022, 17085381211052362. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Sheng, J.; Pan, T.; Wang, Y. Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio are Associated with Lower Extremity Vascular Lesions in Chinese Patients with Type 2 Diabetes. Clin. Lab. 2019, 65. [Google Scholar] [CrossRef]
- Hessami, K.; Tabrizi, R.; Homayoon, N.; Hashemi, A.; Heydari, S.T.; Pour Hosseini, S.A. Gestational diabetes mellitus and inflammatory biomarkers of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio: A systematic review and meta-analysis. Biomarkers 2021, 26, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, A.; Greig, M.; Arshad, M.F.; Julian, T.H.; Tan, S.E.; Elliott, J. Higher admission activated partial thromboplastin time, neutrophil-lymphocyte ratio, serum sodium, and anticoagulant use predict in-hospital COVID-19 mortality in people with Diabetes: Findings from Two University Hospitals in the U.K. Diabetes Res. Clin. Pract. 2021, 178, 108955. [Google Scholar] [CrossRef] [PubMed]
- Mendes, B.B.; Oliveira, A.C.R.; De Alcântara, K.C. Comparison of the neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios in normoglycemic and hyperglycemic subjects. Einstein 2018, 17, eAO4403. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Parameter |
|---|---|
| Gender | Number of Subjects (%) |
| Male | 5938 (41.80) |
| Young | 433 (3.04) |
| Young adults | 2364 (16.64) |
| Adults | 2584 (18.19) |
| Elderlies | 557 (3.92) |
| Female | 8228 (57.92) |
| Young | 429 (3.02) |
| Young adults | 4312 (30.35) |
| Adults | 2862 (20.14) |
| Elderlies | 625 (4.39) |
| Unknown | 39 (0.28) |
| WBC count (×106/mL) | Mean (95% CI) |
| Male | |
| Young | 6.17 (5.98–6.35) |
| Young adults | 6.07 (5.99–6.15) |
| Adults | 6.01 (5.93–6.08) |
| Elderlies | 6.16 (6.00–6.31) |
| Female | |
| Young | 5.92 (5.73–6.12) |
| Young adults | 5.98 (5.92–6.04) |
| Adults | 6.04 (5.97–6.11) |
| Elderlies | 6.02 (5.86–6.17) |
| NLR | Mean (95% CI) |
| Male | |
| Young | 1.24 (1.19–1.30) |
| Young adults | 1.25 (1.22–1.28) |
| Adults | 1.23 (1.20–1.26) |
| Elderlies | 1.30 (1.24–1.37) |
| Female | |
| Young | 1.15 (1.08–1.22) |
| Young adults | 1.24 (1.21–1.26) |
| Adults | 1.26 (1.23–1.29) |
| Elderlies | 1.23 (1.18–1.28) |
| Parameter | NG | IFG | HG |
|---|---|---|---|
| Both genders | |||
| N-NLR | 97.84 | 95.29 | 95.87 |
| H-NLR | 2.16 | 4.71 | 4.12 |
| Males | |||
| N-NLR | 98.14 | 96.08 | 93.33 |
| H-NLR | 1.86 | 3.92 | 6.67 |
| Females | |||
| N-NLR | 97.58 | 94.74 | 91.56 |
| H-NLR | 2.41 | 5.26 | 8.44 |
| Score | 95% CI | z Statistic | p | |
|---|---|---|---|---|
| RR | ||||
| Both genders | ||||
| IFG | 1.68 | 1.50–1.91 | 8.48 | <0.0001 |
| HG | 1.68 | 1.38–2.06 | 5.15 | <0.0001 |
| Males | ||||
| IFG | 1.64 | 1.34–2.02 | 4.82 | <0.0001 |
| HG | 2.60 | 2.09–3.24 | 8.56 | <0.0001 |
| Females | ||||
| IFG | 1.70 | 1.46–1.98 | 6.84 | <0.0001 |
| HG | 2.63 | 2.21–3.13 | 10.92 | <0.0001 |
| OR | ||||
| Both genders | ||||
| IFG | 2.23 | 1.80–2.77 | 7.36 | <0.0001 |
| HG | 1.94 | 1.48–2.56 | 4.79 | <0.0001 |
| Males | ||||
| IFG | 2.15 | 1.51–3.08 | 4.19 | <0.0001 |
| HG | 3.77 | 2.61–5.46 | 7.04 | <0.0001 |
| Females | ||||
| IFG | 2.24 | 1.72–2.93 | 5.94 | <0.0001 |
| HG | 3.73 | 2.81–4.94 | 9.15 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfhili, M.A.; Alsughayyir, J.; Basudan, A.; Ghneim, H.K.; Aboul-Soud, M.A.M.; Marie, M.; Dera, A.; Alfaifi, M.; Alkhathami, A.G.; Awan, Z.A.; et al. Isolated and Combined Effect of Age and Gender on Neutrophil–Lymphocyte Ratio in the Hyperglycemic Saudi Population. Medicina 2022, 58, 1040. https://doi.org/10.3390/medicina58081040
Alfhili MA, Alsughayyir J, Basudan A, Ghneim HK, Aboul-Soud MAM, Marie M, Dera A, Alfaifi M, Alkhathami AG, Awan ZA, et al. Isolated and Combined Effect of Age and Gender on Neutrophil–Lymphocyte Ratio in the Hyperglycemic Saudi Population. Medicina. 2022; 58(8):1040. https://doi.org/10.3390/medicina58081040
Chicago/Turabian StyleAlfhili, Mohammad A., Jawaher Alsughayyir, Ahmed Basudan, Hazem K. Ghneim, Mourad A. M. Aboul-Soud, Mohammed Marie, Ayed Dera, Mohammed Alfaifi, Ali G. Alkhathami, Zuhier A. Awan, and et al. 2022. "Isolated and Combined Effect of Age and Gender on Neutrophil–Lymphocyte Ratio in the Hyperglycemic Saudi Population" Medicina 58, no. 8: 1040. https://doi.org/10.3390/medicina58081040